Come e quando è nato lo Studio DMP-HF
 Lo scompenso cardiaco rappresenta una principale causa di morte e di ricovero ospedaliero nei soggetti anziani, nonostante la disponibilità di cure efficaci. Si tratta di una patologia cronica che va frequentemente incontro a riacutizzazioni per svariati motivi e, quindi, il paziente deve essere continuamente seguito nel suo decorso e inserito in un modello di assistenza multidisciplinare e continuativa.
Lo scompenso cardiaco rappresenta una principale causa di morte e di ricovero ospedaliero nei soggetti anziani, nonostante la disponibilità di cure efficaci. Si tratta di una patologia cronica che va frequentemente incontro a riacutizzazioni per svariati motivi e, quindi, il paziente deve essere continuamente seguito nel suo decorso e inserito in un modello di assistenza multidisciplinare e continuativa.
L’idea di proseguire l’esperienza positiva del gruppo BRAVEHEART con la formazione di un gruppo di lavoro che studiasse l’efficiacia di un modello di gestione multidisciplinare basato sulla valutazione multidimensionale negli anziani con insufficienza cardiaca è nata nel corso delle discussioni e dei lavori preliminari che successivamente hanno portato alla nascita e alla messa a punto del “Documento di Consenso : i percorsi assistenziali del paziente con scompenso cardiaco” e formalizzata durante un incontro tra ricercatori del gruppo BRAVEHEART.
Il presupposto fondamentale si basava sulla carenza di dati attendibili sulla efficacia di un modello Multidisciplinare di gestione ambulatoriale post-dimissione basato sulla VMD in soggetti di età avanzata con scompenso cardiaco, in confronto con un modello convenzionale di cura. L’idea di base è stata la progettazione e la conduzione di un rigoroso studio randomizzato, prospettico finalizzato a produrre evidenze dai e per i pazienti del “mondo reale” della pratica clinica quotidiana che coinvolgesse diversi setting clinici, dalla Cardiologia ospedaliera alle Cure Primarie e diverse figure professionali, come Cardiologi, Infermieri e Medici di Medicina Generale .
Un ruolo non secondario è stato svolto anche dalla comune percezione della necessità di dare una risposta organizzativa efficace ai crescenti bisogni di salute della popolazione anziana affetta da scompenso, in un sistema attualmente ancora frammentato, incapace di offrire continuità di cure.
Infine, come BRAVEHEART, questo gruppo di studio nasce dall’aggregazione spontanea dei suoi componenti e compie le sue ricerche autofinanziandosi e in assoluta indipendenza di programmi da altri organismi privati o pubblici.
Protocollo di Studio di DMP-HF
Lo scopo principale dello studio è stato di implementare e valutare l’efficacia di modelli di assistenza agli anziani con scompenso cardiaco, e, specificamente di un Modello Multidisciplinare.
Nonostante molteplici esperienze pubblicate nell’ultimo decennio a livello internazionale vi è carenza di dati attendibili derivati da studi clinici randomizzati sull’efficacia e sulla costo-efficia di modelli di disease management in soggetti di età avanzata, in particolare quelli fragili, in un sistema sanitario a finanziamento pubblico come quello nazionale.
L’idea di base è stata la progettazione e la conduzione di un trial clinico prospettico randomizzato finalizzato a produrre evidenze dai e per i pazienti del “mondo reale” della pratica clinica quotidiana.
Un ruolo non secondario è stato svolto anche dalla comune percezione della necessità di dare una risposta efficace al quesito se una valutazione multidimensionale eseguita alla visita basale – e finalizzata a definire il profilo di disabilità e di fragilità – possa permettere di selezionare efficacemente fra la popolazione anziana affetta da scompenso cardiaco, quei pazienti che meglio si possano giovare di un determinato modello assistenziale.
L’obiettivo primario include quindi sia un miglioramento degli esiti come morte e/o ricoveri per scompenso cardiaco e per tutte le cause, sia il miglioramento degli indicatori di qualità di cura, sia l’impiego di risorse, valutando se questo modello possa anche permettere di conseguire un risparmio della spesa sanitaria.
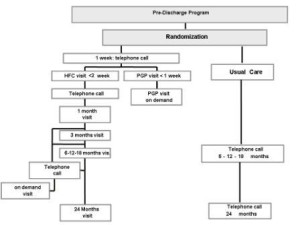
Disegno dello studio e modalità di follow-up
Scarica il Protocollo di Studio
Produzione Scientifica dello studio DMP-HF
Pubblicazioni In Riviste INDEXED peer-reviewed
Two-year outcome of a prospective, controlled study of a disease management programme for elderly patients with heart failure.
Del Sindaco D, Pulignano G, Minardi G, Apostoli A, Guerrieri L, Rotoloni M, Petri G, Fabrizi L, Caroselli A, Venusti R, Chiantera A, Giulivi A, Giovannini E, Leggio F.
J Cardiovasc Med (Hagerstown). 2007 May;8(5):324-9.
OBJECTIVE: Elderly heart failure patients are at high risk of events. Available studies and systematic reviews suggest that elderly patients benefit from disease management programmes (DMPs). However, important questions remain open, including the optimal follow-up intensity and duration and whether such interventions are cost-effective during long-term follow-up and in different healthcare systems. The aim of this study was to determine the long-term efficacy of a hybrid DMP in consecutive older outpatients.
METHODS: Intervention consisted in combined hospital-based (cardiologists and nurse-coordinators from two heart failure clinics) and home-based (patient’s general practitioner visits) care. The components of the DMP were the following: discharge planning, education, therapy optimisation, improved communication, early attention to signs and symptoms. Intensive follow-up was based on scheduled hospital visits (starting within 14 days of discharge), nurse’s phone call and home general practitioner visits.
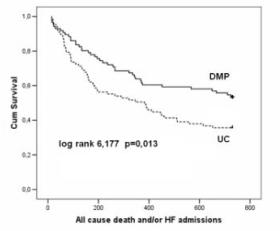
RESULTS: A group of 173 patients aged > or =70 years (mean age 77 +/- 6 years, 48% women) was randomly assigned to DMP (n = 86) or usual care (n = 87). At 2-year follow-up, a 36% reduction in all-cause death and heart failure hospital admissions was observed in DMP vs. usual care. All-cause and heart failure admissions as well as the length of hospital stay were also reduced. DMP patients reported, compared to baseline, significant improvements in functional status, quality of life and beta-blocker prescription rate. The intervention was cost-effective with a mean saving of euro 982.04 per patient enrolled.
CONCLUSIONS: A hybrid DMP for elderly heart failure patients improves outcomes and is cost-effective over a long-term follow-up.
Comment in: Disease management program for the elderly with heart failure. [J Cardiovasc Med (Hagerstown). 2007]
Usefulness of frailty profile for targeting older heart failure patients in disease management programs: a cost-effectiveness, pilot study.
Pulignano G, Del Sindaco D, Di Lenarda A, Tarantini L, Cioffi G, Gregori D, Tinti MD, Monzo L, Minardi G.
J Cardiovasc Med (Hagerstown). 2010 Oct;11(10):739-47. doi: 10.2459/JCM.0b013e328339d981.
BACKGROUND: Disease management programs (DMP) improve outcomes in patients with heart failure. Because older heart failure patients represent a heterogeneous population, the aim of this study was to determine which patients benefit mostly from a DMP, by means of their frailty profile.
SETTING: Heart failure outpatient clinic.
METHODS:Consecutive (n = 173) patients aged more than 70 years were randomized to a multidisciplinary DMP (n = 86) or usual care (n = 87). A modified frailty score (range 1-6) was used as an index of global functional impairment.
RESULTS: Mild to moderate frailty (frailty score = 2-3) was associated with significant improvements in outcomes (death and/or heart failure admission, heart failure admissions and all-cause admissions) in DMP patients vs. usual care. Even in more frail patients (frailty score = 4-6) a significant reduction in heart failure admissions was observed. By contrast, nonfrail patients (frailty score = 1) did not derive significant benefit. In the cost-effectiveness analysis, the mean savings per patient, stratified according to their frailty score, were -1003.31 euro for frailty score 1 (95% confidence interval -3717.00-1709.00), 1104.72 euro for frailty score 2 (-280.6-2491.00), 2635.42 euro for frailty score 3 (352.60-4917.00, P = 0.025) and 419.53 euro for frailty score 4-6 (-1909.00-2749.00). Intervention was therefore significantly cost saving in moderately frail, but not in nonfrail or severely frail patients. Thus, DMP was dominant (i.e. both less costly and more effective than usual care) in moderately frail patients. At sensitivity analysis, DMP remained dominant even to changes in cost of intervention and hospitalizations.
CONCLUSION: This suggests that an intensive, hospital-based DMP appears to be more effective in older patients with mild-to-moderate levels of frailty. Thus, a multidimensional assessment of frailty seems to be a useful tool for appropriate selection of model of care.
Translation and validation of the Italian version of the European Heart Failure Self-care Behaviour Scale.
Pulignano G, Del Sindaco D, Minardi G, Tarantini L, Cioffi G, Bernardi L, Di Biagio D, Leonetti S, Giovannini E.
J Cardiovasc Med (Hagerstown). 2010 Jul;11(7):493-8. doi: 10.2459/JCM.0b013e328335fbf5.
BACKGROUND: Heart failure (HF) patients can benefit from management programmes that include education, discharge planning and structured follow-up. Therefore, it is important to evaluate the improvement of self-care as a result of these interventions. The European Heart Failure Self-care Behaviour Scale (EHFScBS) was developed as a reliable and valid instrument for self-care evaluation.
OBJECTIVES: The aims were to translate and validate the Italian version of the EHFScBS and to evaluate factors related to self-care.
METHODS:The translation and validation were performed as follows: translation and back-translation; evaluation by four bilingual cardiologists; administration to healthy individuals of different ages and education to test language comprehension; final correction by cardiologists experienced in cognitive assessment; and administration in HF patients to test validity and internal consistency.
RESULTS: A sample of 93 HF patients (mean age 77 +/- 6 years, 53% women) was considered for the validation procedure. Fifty-four (58%) patients were already followed in the HF clinic (HFC), with previous HF education, and 39 (42%) were evaluated at baseline. The reliability analysis showed a Cronbach’s alpha of 0.82. At multivariate analysis, age, not already followed in HFC and female sex were associated to worse self-care behaviour. When HFC patients were considered separately, an association between self-care and cognitive dysfunction was observed.
CONCLUSION: The EHFScBS appears to be a valid and reliable instrument in the Italian version also. Self-care behaviour appears to depend on age and sex and a previous HF education. Mild to moderately impaired cognitive function seems to influence self-care in patients who have already received HF education.
PMID: 20407384 [PubMed – indexed for MEDLINE]
The evolving care of the elderly with heart failure: from the ‘high-tech’ to the ‘high-touch’ approach.
Pulignano G, Del Sindaco D, Di Lenarda A, Sinagra G.
J Cardiovasc Med (Hagerstown). 2006 Dec;7(12):841-6.
PMID: 17122668 [PubMed – indexed for MEDLINE]
Chronic renal dysfunction and anaemia are associated with cognitive impairment in older patients with heart failure.
Pulignano G, Del Sindaco D, Di Lenarda A, Tinti MD, Tarantini L, Cioffi G, Tolone S, Pero G, Minardi G.
J Cardiovasc Med (Hagerstown). 2014 Jun;15(6):481-90.
Cognitive impairment, anaemia and chronic kidney disease (CKD) are associated with mortality and disability in chronic heart failure patients. We hypothesized that anaemia and CKD are independent predictors of cognitive impairment in older patients with heart failure.
METHODS: One hundred and ninety community-living elderly patients aged at least 70 years, treated with optimized therapy for heart failure in stable clinical conditions, were prospectively studied. They underwent clinical and multidimensional assessment. Cognitive status was assessed by the Mini Mental State Examination. Cognitive impairment was defined as the Mini Mental State Examination score adjusted by age and educational level below 24. CKD was defined as the Cockcroft-Gault glomerular filtration rate below 60 ml/min and anaemia as haemoglobin below 12 g/dl.
RESULTS: Cognitive impairment was diagnosed in 38.9% of patients, CKD in 85.7% and anaemia in 42.6%. Age, female sex, BMI, education less than 5 years, depressive symptoms, anaemia, CKD, disability and worse quality of life were significantly associated with cognitive impairment. Cognitive impairment involved primarily global cognitive deficit, memory, mental speed, attention, calculation and language. A significant relationship between haemoglobin levels and cognitive impairment was found, with the range of 15-16.5 g/dl having the lower prevalence of cognitive impairment (19.4%). At multivariate analysis, advanced age, low education level, anaemia and CKD were independently associated with cognitive impairment. Cox analysis showed that cognitive impairment was an independent predictor of hospitalization for worsening heart failure alone and combined with all-cause death.
CONCLUSION: Cognitive impairment is common in elderly heart failure patients and is independently associated with anaemia and renal dysfunction. Further studies are needed to assess whether optimal treatment of anaemia and CKD may prevent the development of cognitive impairment in heart failure patients.
Role of a multidisciplinary program in improving outcomes in cognitively impaired heart failure older patients.
Del Sindaco D1, Pulignano G, Di Lenarda A, Tarantini L, Cioffi G, Tolone S, Tinti MD, Monzo L, Barbati G, Minardi G.
Monaldi Arch Chest Dis. 2012 Mar;78(1):20-8.
BACKGROUND: Cognitive impairment (CI) frequently complicates Heart failure (HF) and is associated with increased mortality and morbidity. Previous studies reported that nurse-lead home-based multidisciplinary program (MP) may not improve the prognosis of this high-risk group. In the present study, we analysed the relative effectiveness of an integrated hospital-based MP in patients with cognitive impairment.
METHODS: Consecutive (n = 173) community-living outpatients aged > 70 years (mean 77 +/- 6, 48% women) randomized to a MP (n = 86) or usual care (UC) (n = 87) were enrolled in stable clinical conditions. Cognitive status was assessed by means of Folstein Mini Mental State Examination (MMSE).
RESULTS: CI (MMSE < or = 24) was present in 41.6% (42,5% UC vs 40.7% MP p =ns). The variables independently associated to CI were: older age, education level
CONCLUSIONS: This study suggests that CI is very common and associated to worse prognosis in heart failure and that hospital-based MP seems to improve outcomes in these patients through reduction of heart failure hospital admission.
Two-year outcome of a prospective, controlled study of a disease management programme for elderly patients with heart failure.Del Sindaco D, Pulignano G, Minardi G, Apostoli A, Guerrieri L, Rotoloni M, Petri G, Fabrizi L, Caroselli A, Venusti R, Chiantera A, Giulivi A, Giovannini E, Leggio F.
Division of Cardiology, Cardiogeriatric Department, INRCA Institute of Care and Research, Rome, Italy.
Journal of cardiovascular medicine 2007 May;8(5):324-9.
OBJECTIVE: Elderly heart failure patients are at high risk of events. Available studies and systematic reviews suggest that elderly patients benefit from disease management programmes (DMPs). However, important questions remain open, including the optimal follow-up intensity and duration and whether such interventions are cost-effective during long-term follow-up and in different healthcare systems. The aim of this study was to determine the long-term efficacy of a hybrid DMP in consecutive older outpatients.
METHODS: Intervention consisted in combined hospital-based (cardiologists and nurse-coordinators from two heart failure clinics) and home-based (patient’s general practitioner visits) care. The components of the DMP were the following: discharge planning, education, therapy optimisation, improved communication, early attention to signs and symptoms. Intensive follow-up was based on scheduled hospital visits (starting within 14 days of discharge), nurse’s phone call and home general practitioner visits.
RESULTS: A group of 173 patients aged > or =70 years (mean age 77 +/- 6 years, 48% women) was randomly assigned to DMP (n = 86) or usual care (n = 87). At 2-year follow-up, a 36% reduction in all-cause death and heart failure hospital admissions was observed in DMP vs. usual care. All-cause and heart failure admissions as well as the length of hospital stay were also reduced. DMP patients reported, compared to baseline, significant improvements in functional status, quality of life and beta-blocker prescription rate. The intervention was cost-effective with a mean saving of euro 982.04 per patient enrolled.
CONCLUSIONS: A hybrid DMP for elderly heart failure patients improves outcomes and is cost-effective over a long-term follow-up.
Scarica gli abstarct dei lavori da PubMed
- Pulignano G, Del Sindaco D, Di Lenarda A, Tarantini L, Cioffi G, Gregori D, Tinti MD, Monzo L, Minardi G.
Usefulness of frailty profile for targeting older heart failure patients in disease management programs: a cost-effectiveness, pilot study.
J Cardiovasc Med (Hagerstown). 2010 Oct;11(10):739-47. >Abstract disponibile< - Pulignano G, Del Sindaco D, Minardi G, Tarantini L, Cioffi G, Bernardi L, Di Biagio D, Leonetti S, Giovannini E.
Translation and validation of the Italian version of the European Heart Failure Self-care Behaviour Scale.
J Cardiovasc Med (Hagerstown). 2010 Jul;11(7):493-8. >Abstract disponibile< - Del Sindaco D, Pulignano G, Minardi G, Apostoli A, Guerrieri L, Rotoloni M, Petri G, Fabrizi L, Caroselli A, Venusti R, Chiantera A, Giulivi A, Giovannini E, Leggio F.
Two-year outcome of a prospective, controlled study of a disease management programme for elderly patients with heart failure.
J Cardiovasc Med (Hagerstown). 2007 May;8(5):324-9. >Abstract disponibile<
Abstracts a congressi internazionali
- D. Del Sindaco, G. Pulignano, A. Giulivi, G. Minardi , A. Chiantera, A. Lorettu, L. Guerrieri, A. Apostoli, F. Leggio, E. Giovannini. 2-year outcome of a prospective, controlled study on the effects of a multidisciplinary management program for elderly with heart failure. Eur J Heart Fail 2004; 3 (suppl1 ): 31.
- G. Pulignano, D. Del Sindaco, A. Giulivi, G. Minardi , A. Apostoli, M.Rotoloni, F. Leggio, E. Giovannini. Effects of a multidisciplinary management program for elderly with heart failure. 2-year outcome of a prospective, controlled study. Eur Heart Journal 2004 (abst.supplement): 440
- Del Sindaco, G. Pulignano, A. Di Lenarda, M. Merlo, G. Cioffi , L. Tarantini, M. Leggio, G. Sinagra , E. Giovannini, F. Leggio. Impact of anemia and renal dysfunction on cognitive function in elderly patients with heart failure. Eur J Heart Failure 2005; 6: abstr suppl: 156.
- G. Pulignano, D. Del Sindaco, A. Di Lenarda, A. Giulivi, M. Merlo, G. Cioffi, L. Tarantini, G. Minardi, G. Sinagra, E. Giovannini. Prognostic importance of anemia in very elderly patients with heart failure on optimized therapy. Eur J Heart Failure 2005; 6: abstr suppl: 196.
- Del Sindaco, G. Pulignano, A. Di Lenarda, M. Merlo, G. Cioffi , L. Tarantini, M. Leggio, G. Sinagra , E. Giovannini, F. Leggio. Impact of anemia and renal dysfunction on cognitive function in elderly patients with heart failure. European Heart Journal 2005;Vol.26(Abstract Supplement):501.
- G Pulignano, D Del Sindaco, A Di Lenarda, G Cioffi, L Tarantini, F Leggio, G Sinagra, E Giovannini. Frailty is an independent prognostic variable in very elderly patients with heart failure. Eur J Heart Fail 2006; 7(Abstract Suppl) (Oral presentation)
- D Del Sindaco, G Pulignano, A Di Lenarda, G Minardi, C Manzara, G Sinagra, E Giovannini, E Leggio Frailty is strongly associated to cardio-renal-anemia syndrome in elderly community-living heart failure patients. Eur J Heart Fail 2006; 7(Abstract Suppl).
- G. Pulignano, D. Del Sindaco, A. Di Lenarda, G. Cioffi, C. Manzara, F. Leggio, G. Sinagra, E. Giovannini. Frailty is an independent prognostic variable in very elderly patients with heart failure. Eur Heart J 2006; 27(Abstract Suppl), 22.
- G Pulignano, D Del Sindaco, A Di Lenarda, L Tarantini, G Cioffi, , C.Manzara, D.Gregori, G.Minardi. Are disease management programs cost-effective for all elderly patients with heart failure? Usefulness of frailty profile in selection process, a randomised study . Eur J Heart Failure 2007 (abstr.suppl).
- G Pulignano, D Del Sindaco, A Di Lenarda, L Tarantini, G Cioffi, , C.Manzara, D.Gregori, G.Minardi. Are disease management programs cost-effective for all elderly patients with heart failure? Usefulness of frailty profile in selection process, a randomised study . Eur Heart J 2007 (abstr.suppl).
Abstracts a congressi nazionali
–